Anotia or clinical anotia
The case with no auricle congenitally is called anotia. Even though a small lobule or an accessory auricle exists, it is to be excised if it is located far from the planned reconstruction site; after the excision, there exists no auricle and thus this is called clinically anotia. Performing the auricle reconstruction with the traditional procedures was believed impossible for the cases of anotia or clinical anotia, due to the insufficient skin surface area. Furthermore, the auricle reconstruction for anotia complicated with low hairline was believed even more impossible. With the Nagata method, however, such difficult issues related to anotia are solved by its procedures of hair follicle removal, 3-D costal cartilage graft and then TPF cover followed by ultra-delicate split thickness scalp skin [UDSTS] cover, and consequently, the auricle reconstruction for anotia is successfully realized on the normal location.

Severe low hairline case, which makes the auricular reconstruction
very complicated and difficult

Preoperative appearance
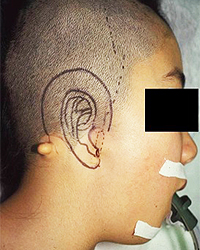
1st stage pre-operative appearance
Design (The auricular reconstruction site penetrates into the hair bearing skin.)
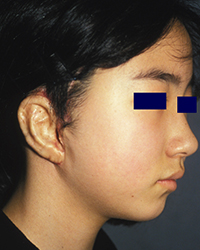
2nd stage post-operative appearance

2nd stage post-operative appearance
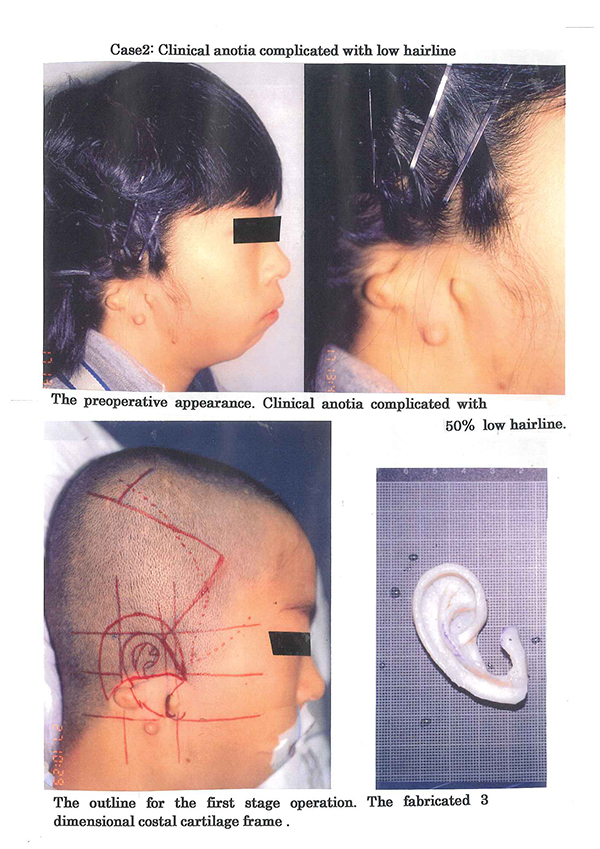
Before the operation:
Generally the vast majority of the anotia cases are associated with low hairline thus making auricular reconstruction complicated and difficult. Especially, the anotia case with severe low hairline as shown in the photo requires more complicated procedures.
During the first-stage operation:
The operative outline for the first stage operation reveals that 75% of the auricular reconstruction site penetrates into the hair bearing skin.
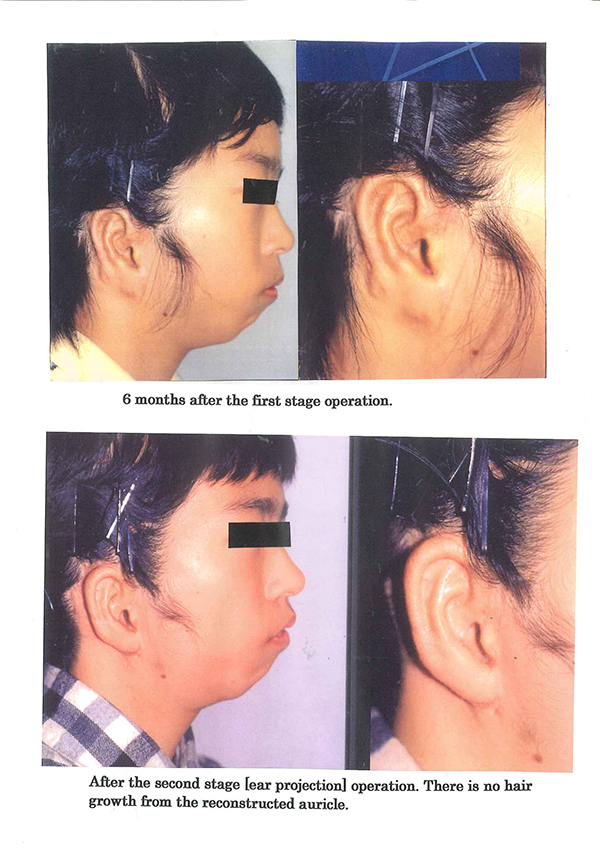
After the second-stage operation:
There is no hair growth on the reconstructed auricle. It is possible to properly reconstruct and project the auricle even in anotia cases complicated with low hairline.
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
First stage operation-The fabrication of the 3 dimensional costal cartilage frame [3-D frame]
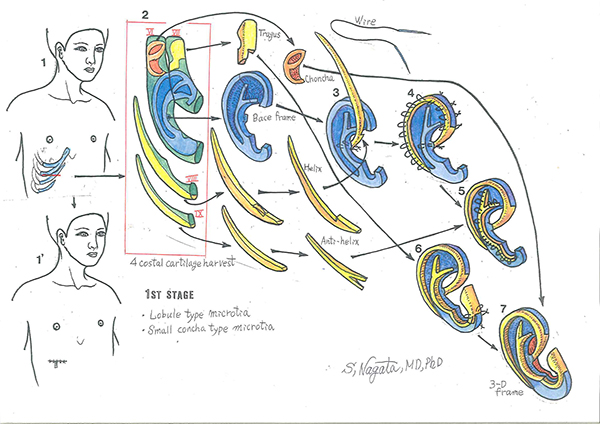
Diagram 1: The costal cartilages harvested for the fabrication of the 3-D frame are the sixth, seventh, eights, and the ninth costal cartilages. Diagram 2: Harvested 4 costal cartilages. The tragus unit, the base frame units, the crus helices-helical rim unit and the superior and inferior crus antihelix unit are fabricated from the costal cartilages. The units for the fabrication of the base frame; these units are fabricated from the sixth and seventh costal cartilages with 38 gauge stainless steel double-armed wire sutures. Diagram 3: The head of the proximal region of the crus helicis is fixed to the posterior surface of the base frame and the notch is aligned to the base flame to reinforce the strength of the 3-D frame. Diagram 4: Wire fixations are placed 3 mm intervals. Note that the loop portion of the wire sutures is embedded into the cartilage framework to avoid the postoperative complication of wire suture protrusion. Diagram 5: The fixation of the superior and inferior crus-antihelix unit, commencing from the superior crus, inferior crus, to the antihelix. Diagram 6: The appearance after the fixation of the tragus unit. Diagram 7: The appearance after the fixation of the conchal vault unit and completely fabricated 3-D frame.
The first-stage operation for clinical anotia complicated with low hairline
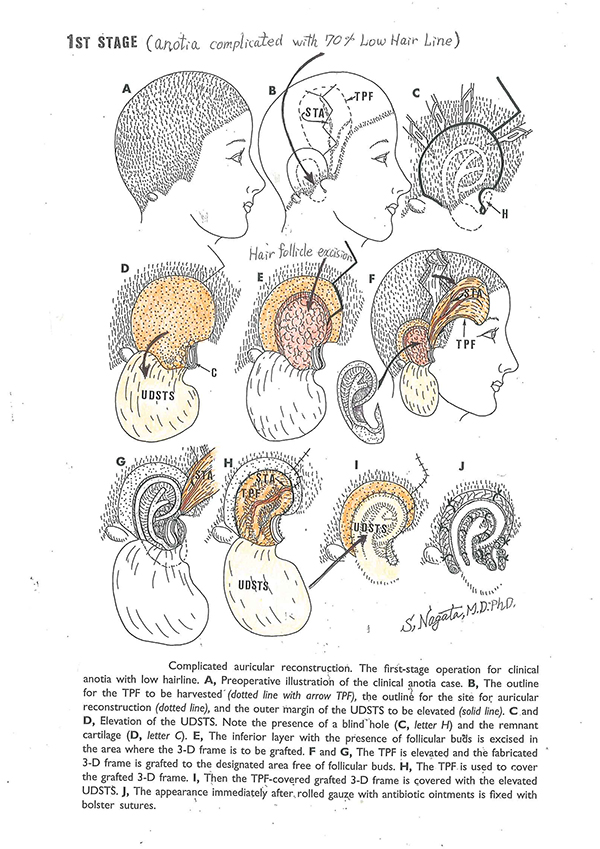
The preoperative appearance is illustrated in Diagram A, and from the outline for auricular reconstruction [see Diagram B and C], over 70% of the surgical site for auricular reconstruction is covered with hair growth [low hairline]. To secure ample skin surface area to cover the fabricated 3-D frame, the area 15 to 20 mm from the anatomic outline of the auricle to be constructed is elevated as UDSTS [see Diagram: C and D]; note that the UDSTS is free of follicular buds. The subepidermal layer with the follicular buds is to be excised only in the area to which the 3-D frame is to be grafted [see Diagram E to G], or else postoperative hair growth is expected to occur from the constructed auricle. The TPF is elevated to cover the anterior surface of the grafted 3-D frame [see Diagram F to H], and then the TPF is covered with UDSTS [see Diagram I].
The second-stage operation for clinical anotia complicated with low hairline
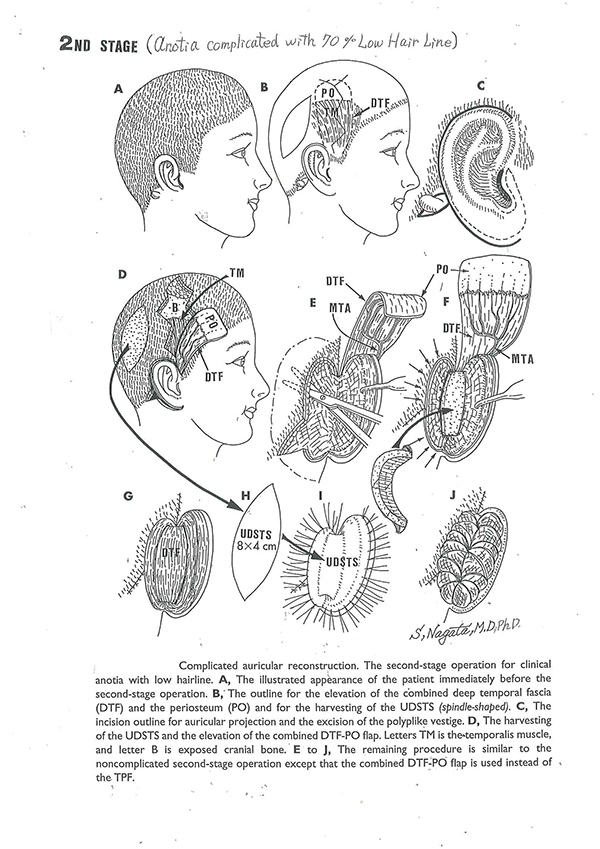
The schematic illustration of the second stage operation is shown. Because the TPF was used to cover the grafted 3-D frame in the first-stage operation, the deep temporal fascia flap [DTF] and periosteum [PO] combined flap is used to cover the posterior surface of the posterior auricle, costal cartilage block, and mastoid surface. All the other surgical procedures are the same as for the non-complicated second-stage operation for auricular reconstruction.
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.

Click here for “Clinical anotia complicated with low hair line” conducted on Feb. 10, 2015 for your reference.