Home > Accuracy evaluation on proportions of the reconstructed auricle / microtia surgery.
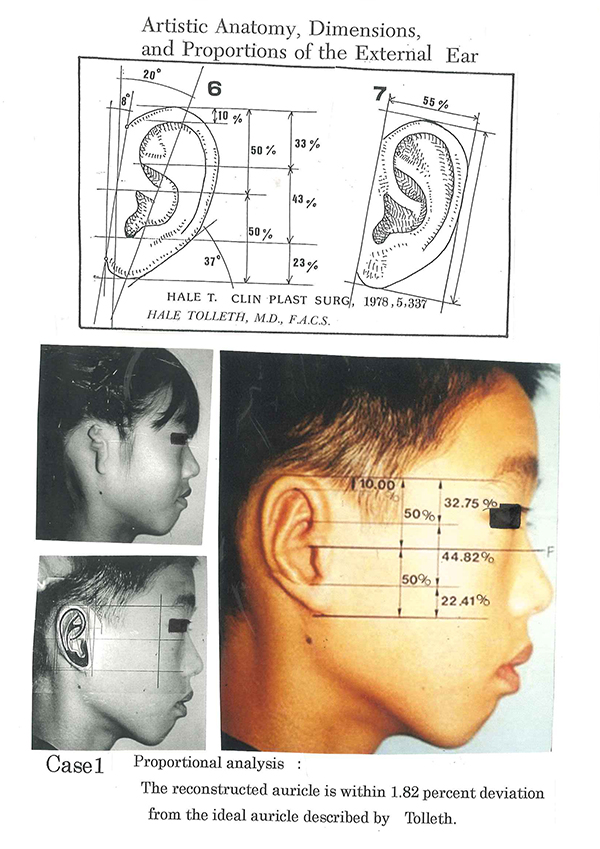
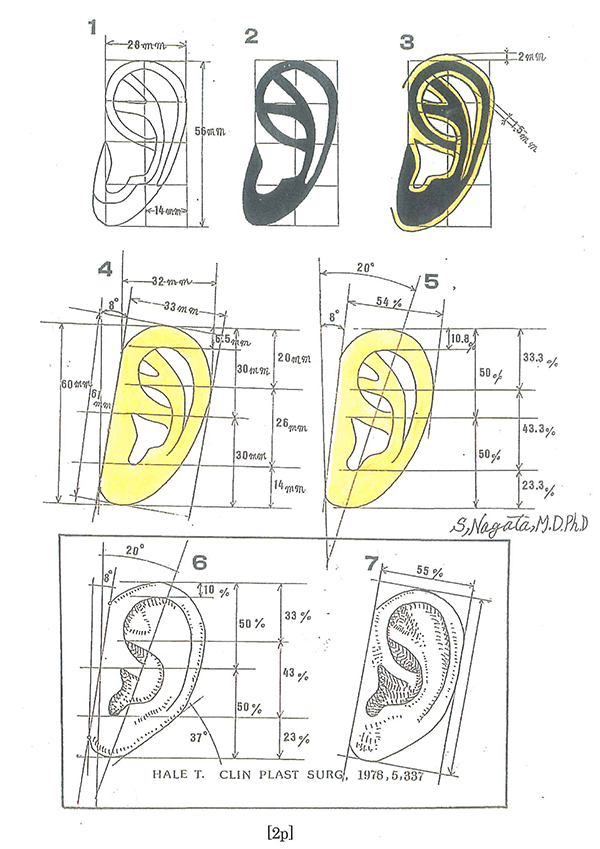
In 1978, HALE TOLLETH published a paper titled Artistic Anatomy, Dimensions, and Proportions of the External Ear in CLIN PLAST SURG, 1978 Jul;5(3):337-45 and reported about ideal auricular morphology with illustration.
In other words, he analyzed ‘ideal auricular morphology in terms of proportions’ and reported it in the paper.
This paper is still famous and must-read for plastic surgeons conducting ear reconstruction surgeries.
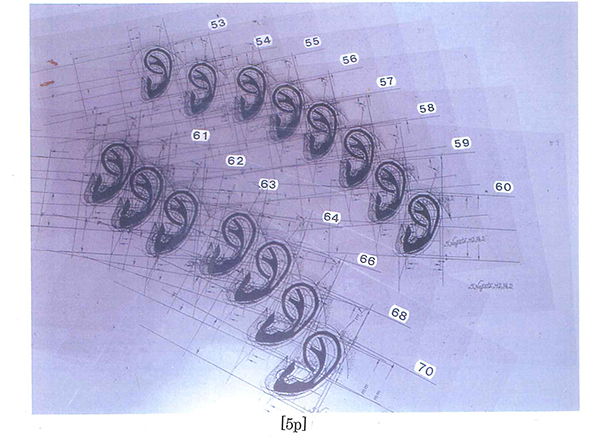
Ears reconstructed by plastic surgeons can be evaluated with percent error for morphological accuracy based on the result shown on this paper.
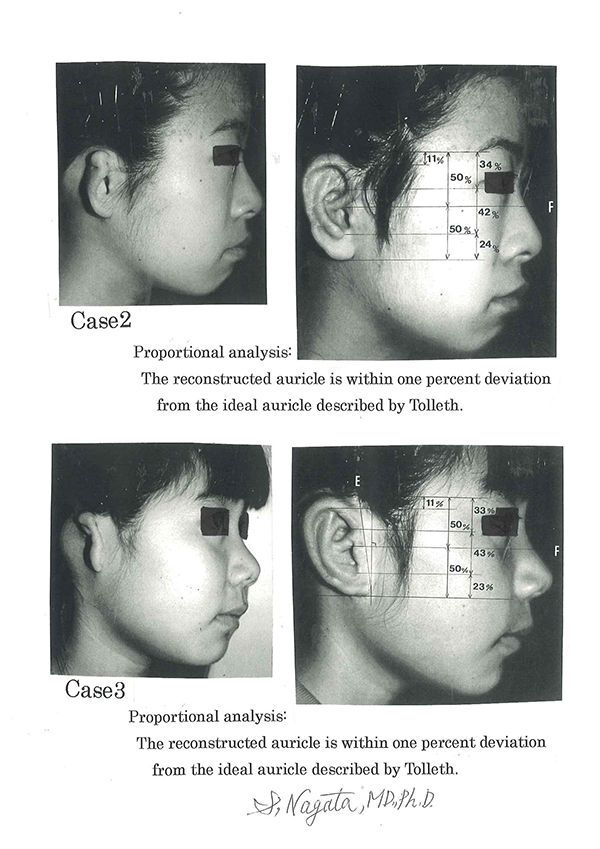
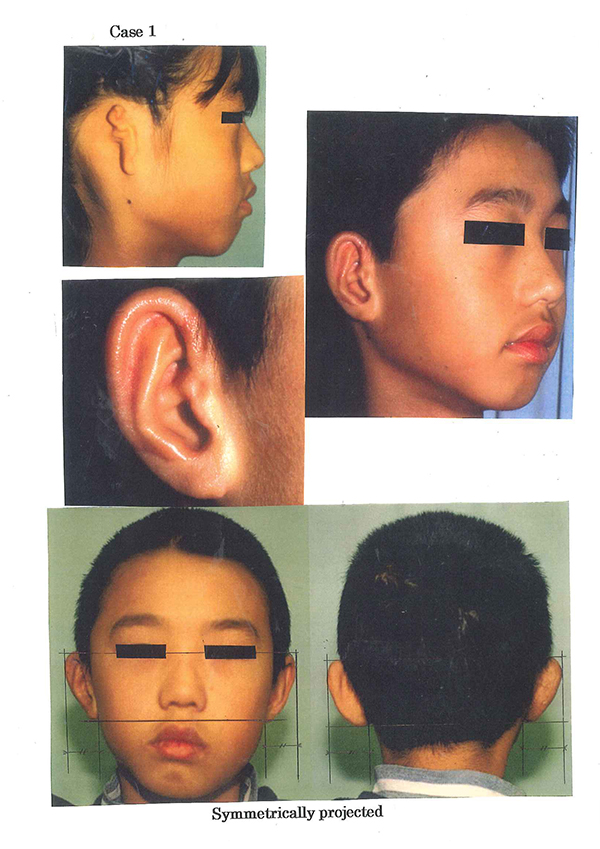
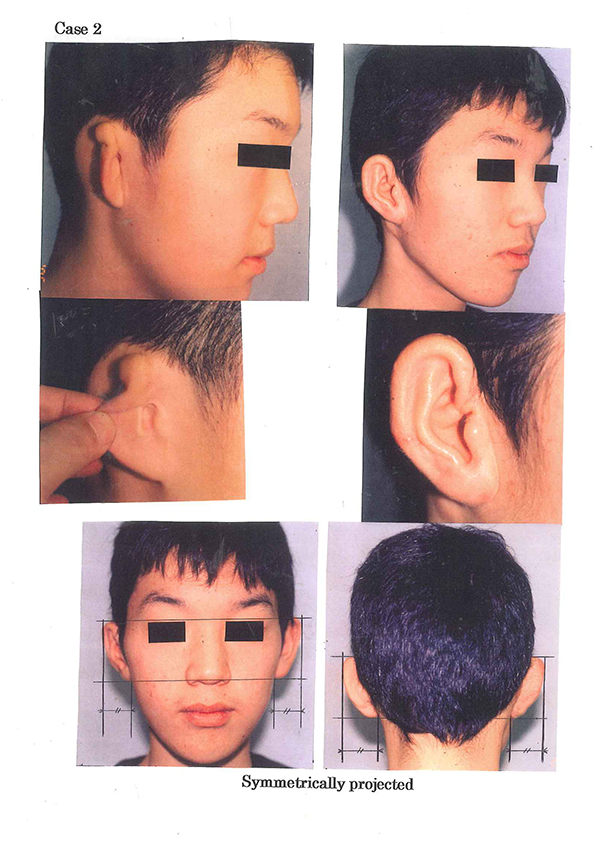
Percent error for ears reconstructed with Nagata method is found to be 1% or within 2% deviation compared to the HALE TOLLETH’s ideal auricular proportions as shown on the photos below.
Those errors stay within almost 1 mm when converted to the actual length.
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Planning for auricular reconstruction with ideal proportions
◆ Paper surgery of ear reconstruction
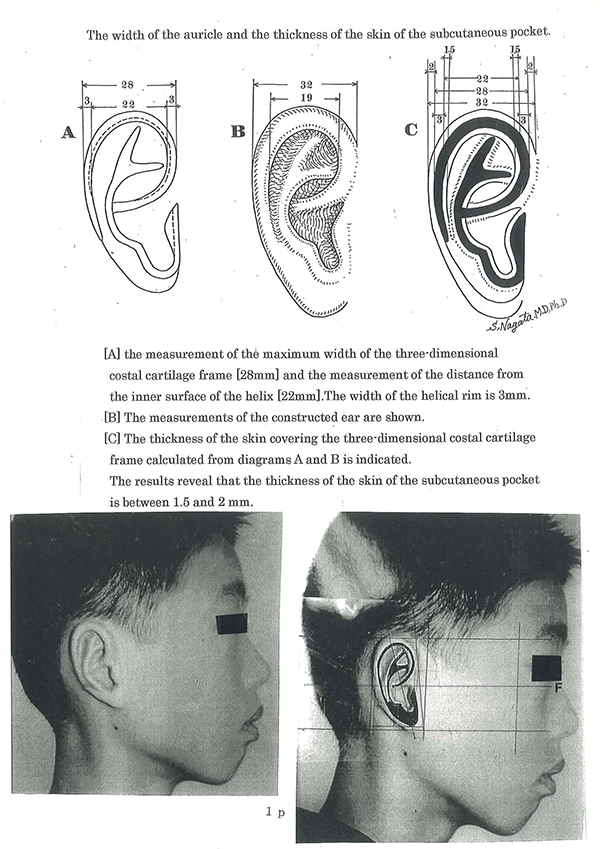
Diagram 1 is the paper template for the fabrication of the three-dimensional costal cartilage framework [3-D frame], Diagram 2 is colored black and Diagram 3 shows the skin cover [shaded yellow].
Note that the lateral thickness of the skin cover is 2mm and the medial surface 1.5mm as reported in [page 1] the PRS in 1994.
The proportional analyses of an ideal auricle described by Tolleth is shown in the lower panel and the proportional and dimensional analyses of the reconstructed auricle [shaded yellow] is calculated on paper, a form of paper surgery.
Note that the calculated results [center panel] are almost identical to that reported by Tolleth.
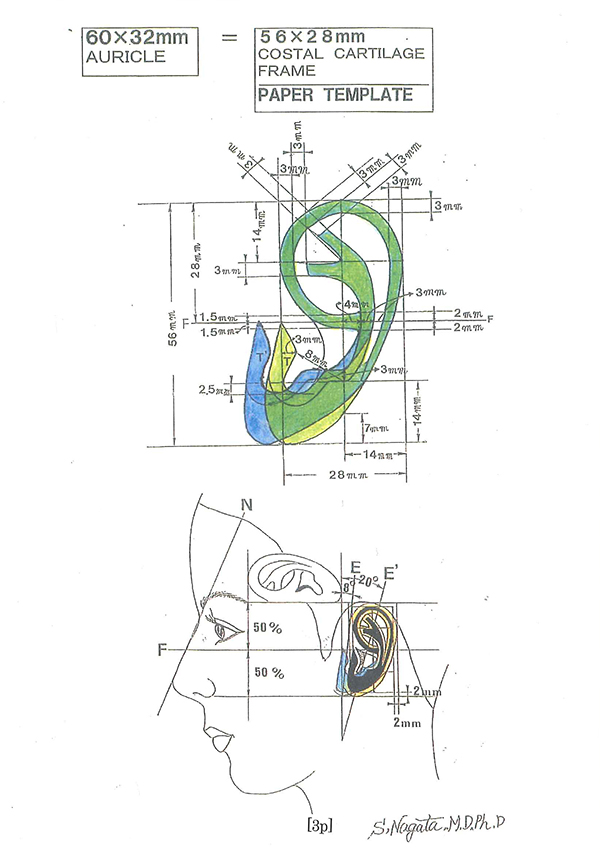
◆ Paper template
On the upper illustration, the fabrication of the paper template for a 60mm 3-D frame is illustrated where the actual length is 56mm due to the consideration of the skin cover.
The tragus is shaded green and blue.
This is to match the width of the auricle to be reconstructed to be identical to the opposite normal auricle in unilateral cases.
The lower panel shows the proper anatomical location where the auricle is to be reconstructed.
The letter F is the Frankfurt Horizontal Line.
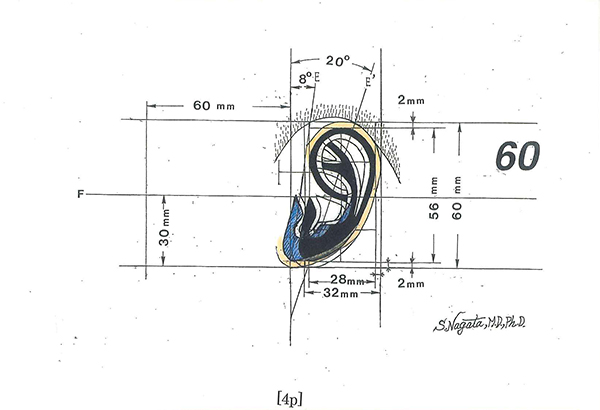
◆ Transparent film template
The transparent film template is to identify the proper anatomical location. The letter F is the Frankfurt Horizontal Line.
A full range of film templates can easily be constructed with a photocopier. As for unilateral cases, after determining the size of the 3-D frame from the normal opposite auricle, the lateral margin of the eyebrow and eye are marked.
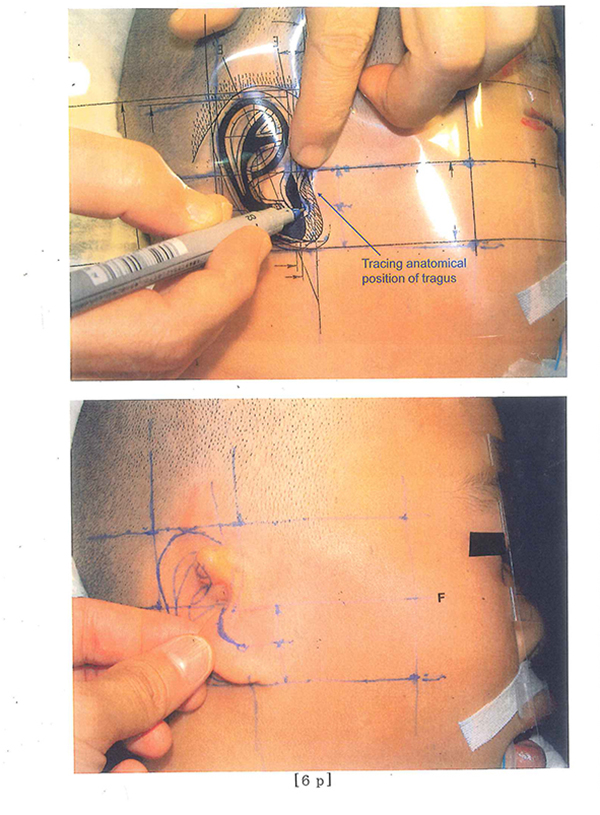
Determine the proper anatomical location during the first stage operation with the transparent film template. The film template is reversed and the markings are aligned to the eyebrow and eye. The tragus is specifically designed for each patient.
Careful and precise preoperative planning is essential. The outline from the film template is traced unto the patient.
[Upper photo]
The actual outline for the reconstruction of the auricle and the anterior surface of the lobule. [Lower photo]
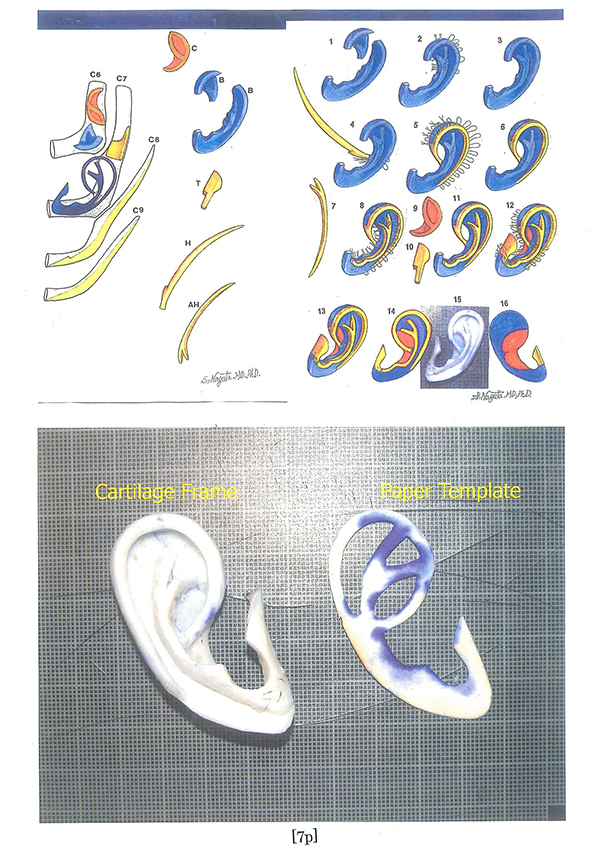
[Upper photo]
The schematic illustration on how the 3-D frame units are fabricated is shown on the left and how the 3-D units are fixed with 38 gauge double armed wire sutures on the right. Paper template is useful for fabrication of the 3-dimensional costal cartilage framework.
[Lower photo]
The fabricated 3-D frame and the paper template.
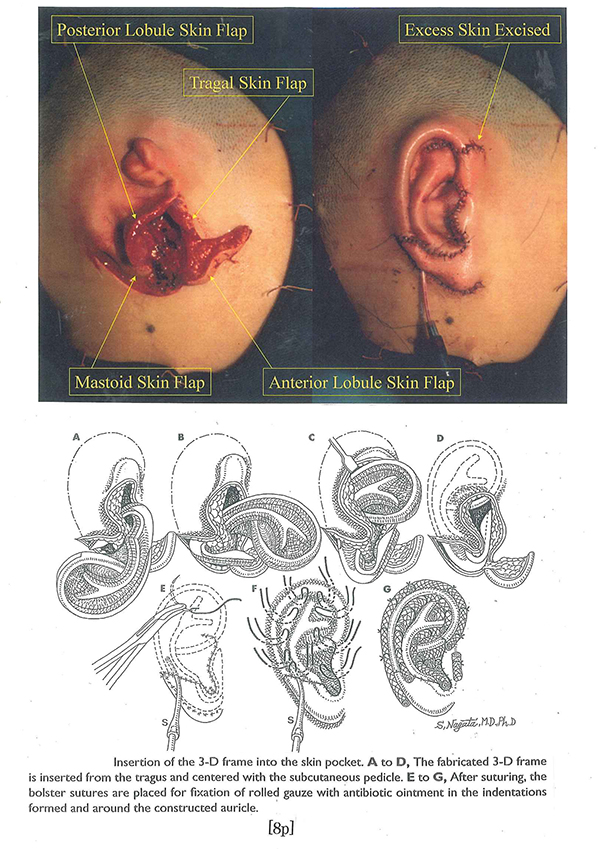
[Upper photo]
The intraoperative appearance with the skin flaps formed [tragus skin flap, posterior and anterior skin flaps of the lobule and mastoid skin flap] and immediately after the first stage operation prior to Bolster sutures. Note that the excess skin in the anterior region of the helical rim is excised during the first stage operation.
[Lower illustration]
The schematic illustration showing how the 3-D frame is inserted into the skin pocket.
The 3-D frame is inserted from the tragus and centered with the subcutaneous pedicle.
After suturing, Bolster sutures are placed into the indentations and around the helical margin as shown.
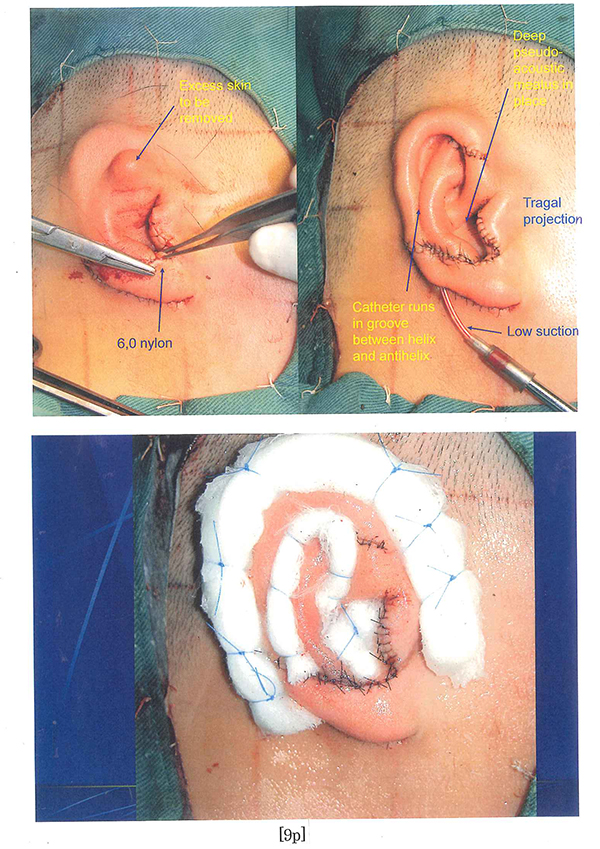
[Upper photo]
The actual intraoperative appearance after insertion of the 3-D frame into the skin pocket. On the right, suction is applied to visualize the contour of the reconstructed auricle.
[Lower photo]
The actual appearance at the end of the first stage operation with Bolster sutures.
Suction drains are not used because, with Nagata method, unlike the Tanzer or Brent method where skin surface area is insufficient, there is ample and sufficient skin surface area to cover the 3-D frame. Therefore it is possible to use the Bolster sutures without the worry of necrosis.
“Knowledge required for auricular reconstruction for microtia and symmetrical projection of the reconstructed auricle”
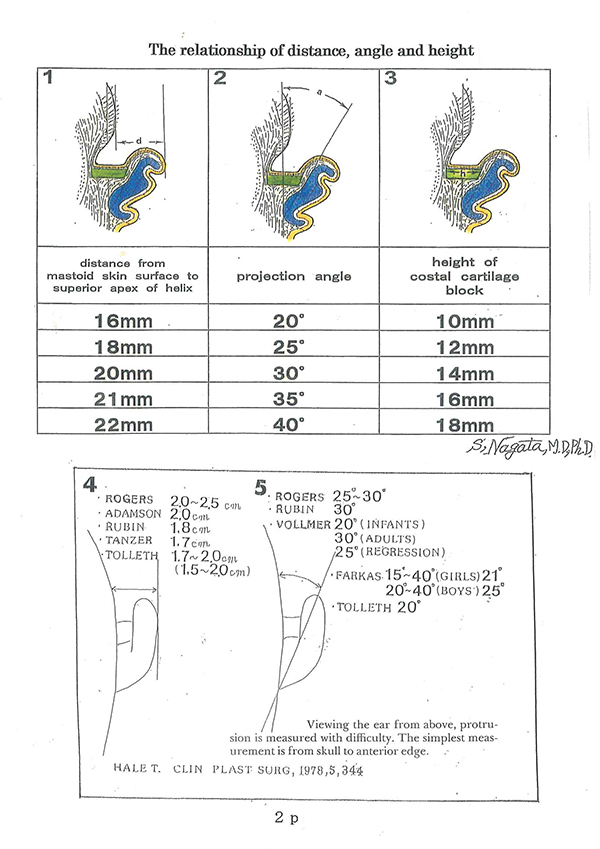
It is really difficult to measure the accurate angle of auricular projection, though the angle of normal auricular projection has been reported variously from 15 to 40 degrees. See Page 2, Figure 5.
On the other hand, the distance from superior apex of auricle to scalp (mastoid skin surface) is measurable, which has been reported variously from 15 to 25 mm. See Page 2, Figure 4.
In addition, we had had no such academic papers that reported and explained “the relationship of the distance from superior apex of helix to scalp, the angle of auricular projection and the height of costal cartilage block grafted to the posterior surface of the reconstructed auricle.”With the conventional methods such as Tanzer, Brent or others, it was impossible to symmetrically project the auricle reconstructed with costal cartilage graft.With Nagata method, at the second stage operation of ear projection, the costal cartilage block is grafted to the posterior surface of the reconstructed auricle to support and symmetrically project the auricle. Then, in order to make the grafted costal cartilage survive and also to improve blood circulation in the projected auricle that has less blood circulation due to the release from head, the entire back of the auricle is covered with good blood circulation of temporoparietal fascia flap (TPF),followed by ultra-delicate split-thickness scalp skin (UDSTS).
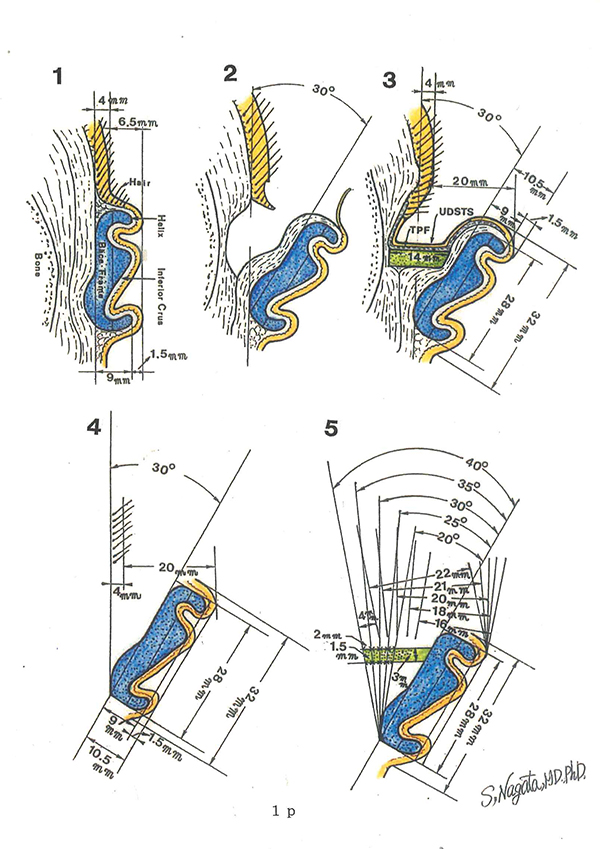
The surgeon needs to know in advance the height of costal cartilage block required to project the reconstructed auricle symmetrically. Page 1, Figure 1 is an illustration of the auricle after the first stage operation of costal cartilage graft for microtia. Page 1, Figure 2 is an illustration of the reconstructed auricle released from head and projected with 30 degrees. Page 1, Figure 4 shows the pattern diagram which derives the relationship of the angle of auricular projection of 30 degrees to the distance from scalp to the highest plane of the reconstructed auricle of 20 mm. As shown in Page 1, Figure 3, the height of 14 mm of costal cartilage block is necessary as a graft fixed between auricle and head for support in order to keep the angle of 30 degrees for auricular projection.
The pattern diagram on Page 1, Figure 5 shows that a change of 2 mm in the height of grafted costal cartilage block results in 5 degree change in the angle of auricular projection. A change in angle of projection of 5 degrees reveals that the distance from auricle to scalp changes by 1 mm increase for the projection angles over 30 degrees and by 2 mm decrease for the projection angles less than 30 degrees.
The relationship mentioned above is tabulated on Page 2, Figure 1, 2 and 3. The relationship of the distance from superior apex of auricle to scalp, angle of auricular projection and the height of costal cartilage block grafted to the posterior surface of the reconstructed auricle is 20 mm, 30 degrees and 14 mm respectively. In the same way, when the angle of auricular projection is 25 degrees, then the distance and the height of costal cartilage block grafted are determined to be 18 mm and 12 mm respectively, and when the angle of auricular projection is 35 degrees, then the distance and the height of costal cartilage block grafted are determined to be 21 mm and 16 mm respectively.
It is extremely important that the plastic surgeon performing microtia surgeries fully comprehends the relationship mentioned above in order to attain symmetrical projection of the reconstructed auricle.
Here are the representative cases of microtia auricles reconstructed symmetrically with Nagata method.
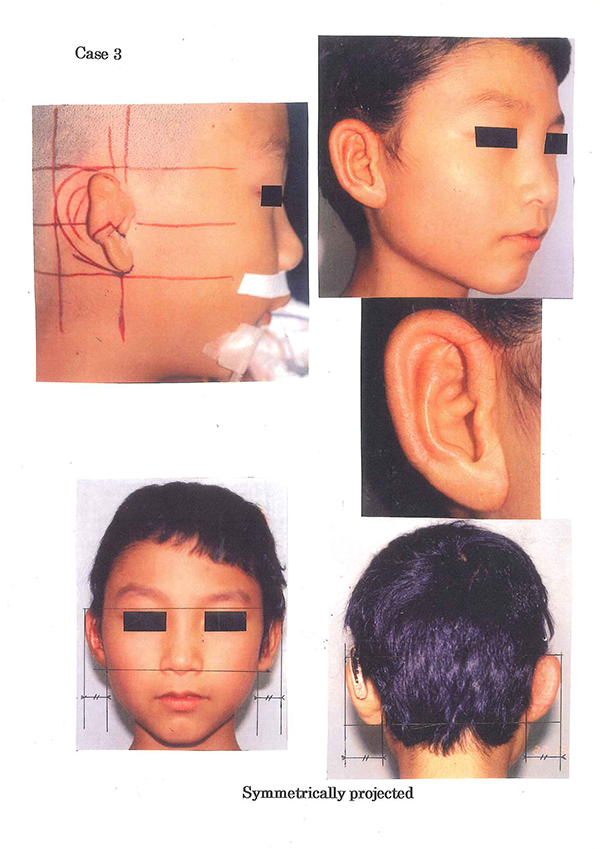
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.