Home > Auricular Reconstruction Nagata Method
Summary
1.
Microtia is the most well-known congenital anomaly of the auricle, and it results from incomplete embryonic development.
2.
Auricular reconstruction for congenital auricular anomalies is based on the degree of severity of the auricular defect in comparison to the opposite normal auricle in unilateral cases.
3.
Classification of congenital auricular defects is clinically divided into: [1] lobule type microtia; [2] small concha type microtia; [3] concha type microtia; [4] anotia and [5-8] those with low hairline.
4.
It is extremely important that the surgeon attempting to reconstruct the auricle fully comprehends its three-dimensional [3-D] morphologic features.
5.
The best material for fabrication of the 3-D framework is autogenous costal cartilage because of the least number of postoperative complications.
6.
The criteria for auricular reconstruction are: [1] the patient is to be over 10-years-old; and [2] the chest circumference at the level of the xiphoid process is to be at least 60 cm.
7.
The first stage operation is the fabrication and grafting of the three-dimensional costal cartilage framework [3-D frame] and the second stage operation is the projection of the reconstructed auricle.
8.
It is important to comprehend the relationship between the angle of projection, distance from the temporal surface to the highest plane of the auricle and the height of the cartilage construct for a successful and symmetrical projection of the reconstructed auricle.
9.
With the use of the temporoparietal fascia flap [TPF] and ultra-delicate split thickness scalp skin [UDSTS] during the first stage operation, the problems created by low hairline have been resolved, and the surgical results have been consistent and satisfactory.
10.
Skin grafting alone for auricular reconstruction is contraindicated.
About MRI examination
Nagata 38 Gauge Microtia Wire is made of stainless steel. About 80 pieces of wire sutures are used at the fabrication of 3-D framework and about 20 pieces at the fabrication of costal cartilage block for ear projection.
We used to tell patients not to take MRI exams after the mictoria reconstructive operation, however, there was an interesting presentation reported at the ISAR meeting at Beijing, China in September, 2017, in which an evaluation of MRI safety was conducted for surgical steel sutures used for microtia reconstruction including Nagata 38 Gauge Microtia Wire and its conclusion is cited as below:
* Conclusions: The steel sutures that underwent testing do not present additional risks to patients in a 3-Tesla or less MRI setting (i.e., MR Conditional). Artifacts for these sutures may only be an issue within close proximity to the reconstructed ear.
* Cited from the abstract presented by Tania L. Kraai, M.D. at ISAR Meeting 2017 in Beijing, China.
It is recommended to consult with your physician explaining about a hundred of wire sutures are embedded in your ear framework before taking any MRI exams.
Nagata Microtia and Reconstructive Plastic Surgery Clinic
Criteria for surgery
Auricular reconstruction is generally performed at the age of 10 years due to volume of costal cartilage required for the fabrication of a sturdy and rigid 3 dimensional costal cartilage frame [3-D frame]. Also, the size of the auricle at 10years of age is approximately the size of an adult. The criteria that I established for auricular reconstruction are: [1] the patient should be 10-years-old; and [2] the chest circumference at the level of the xiphoid process is to be at least 60 cm.
Auricular Reconstruction Nagata Method
The Nagata Auricular Reconstruction Method is a two-stage total auricular reconstruction where the first stage operation involves the harvesting of the costal cartilages, fabrication of the three-dimensional costal cartilage framework (3-D frame) and the grafting of the 3-D frame to its proper anatomical location.
The second stage operation is the elevation of the reconstructed auricle to match the projection of the opposite normal auricle in unilateral cases and to project the auricle to the ideal angle of projection for bilateral cases. Representative primary auricular reconstruction cases performed with Nagata Method are shown below (case 1-7). For cases requiring secondary auricular reconstruction for unfavorable primary auricular reconstruction results at other institutions are represented by case 8-11. Most auricular reconstruction cases are primary auricular reconstruction but presently the number of secondary auricular reconstruction cases is rapidly increasing not only domestically but internationally.
Incision line for the costal cartilage harvest
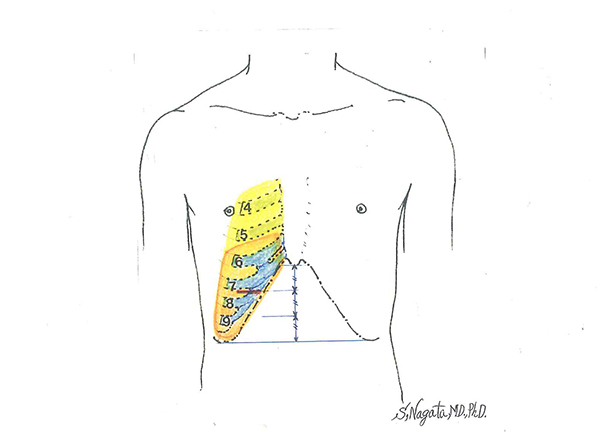
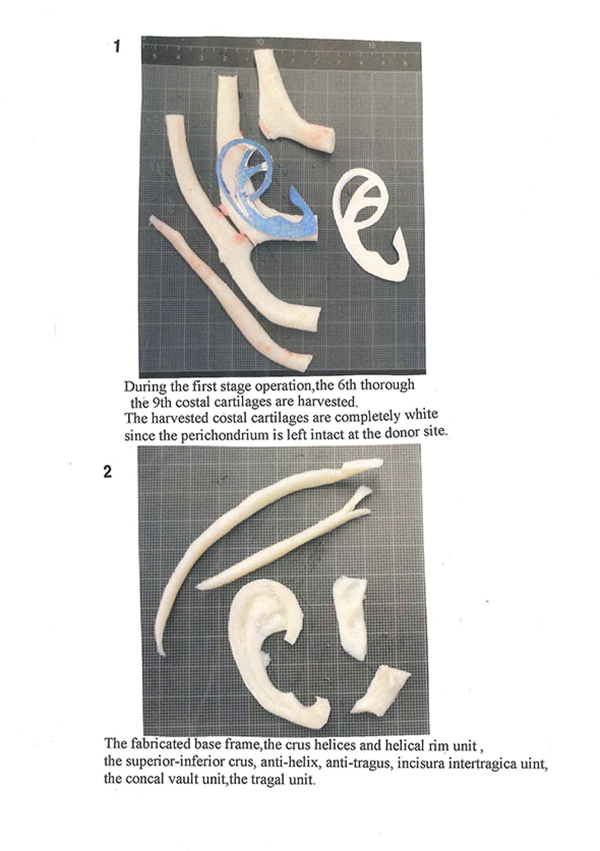
Divide the length from the xiphoid process to the inferior margin of the costal cartilage to three and draw a horizontal line one third from the top. That is approximately where the inferior margin of the 7th costal cartilage is. The horizontal incision line is 5 cm. During the first stage operation, the 6th through the 9th costal cartilages are harvested. During the second stage operation, the 4th and 5th costal cartilages are harvested.
Harvested costal cartilages
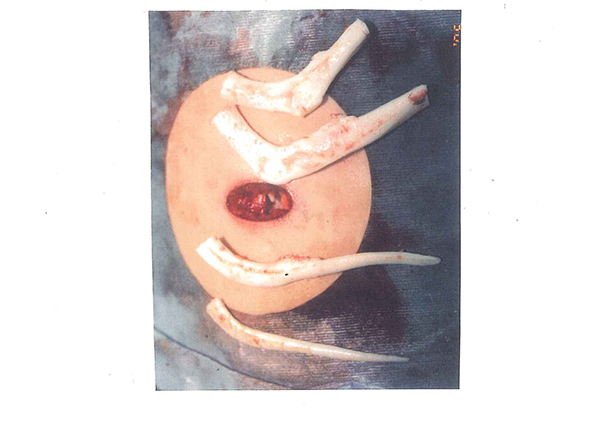
The costal cartilages harvested en block. Note that they are completely white in color, since the perichondrium is left completely intact at the site of harvest. In addition, as shown here, the harvested costal cartilage will differ from case to case. The costal cartilages are harvested through a short incision. With this Nagata method of costal cartilage harvest one need not worry about postoperative chest wall deformity and the scar is greatly minimized.
Harvesting of the costal cartilages
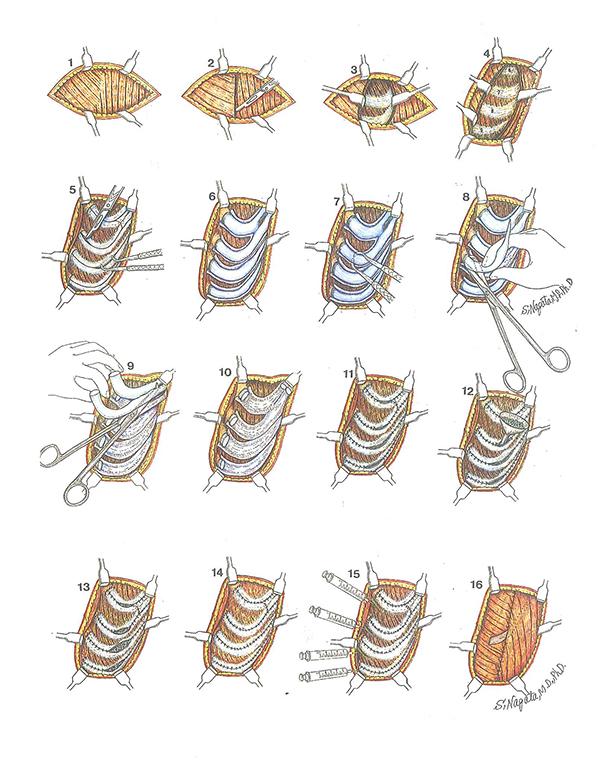
The skin and fat are incised, and the fascias of the external abdominal oblique muscle and rectus abdominis muscle are exposed [Diagram 1]. Incise between the two muscles [Diagram 2] and the intercostal muscle and perichondrium of the 6th through 9th costal cartilages appear [Diagram 3, 4]. Mark the center of the perichondrium, and cut with scalpel and undermine anterior perichondrium open using perichondrial elevator [Diagram 5, 6]. And posterior perichondrium undermine using perichondrial elevator [Diagram 7]. For the 8th and 9th costal cartilages hold the cartilage and cut slightly the cartilage side of the costochondral junction using a costal cartilage cutter [Diagram 8]. The 6th and 7th costal cartilages are harvested en bloc because they tend to be in junction with each other [Diagram 9]. After harvesting all the cartilages, the perichondrium is left open [Diagram 10]. Suture with 4-0 nylon at 5 mm intervals but leave the central portion open [Diagram 11]. From there, return the remaining cartilages that have been diced to 2 to 3 mm blocks using a funnel until the perichondrium is full [Diagram 12, 13]. Then suture the rest of the perichondrium [Diagram 14]. Because the perichondrium is left completely at the donor site there is no chest deformity. The returned cartilage will regenerate over time.
The fabrication of the 3 dimensional costal cartilage frame [3-D frame]
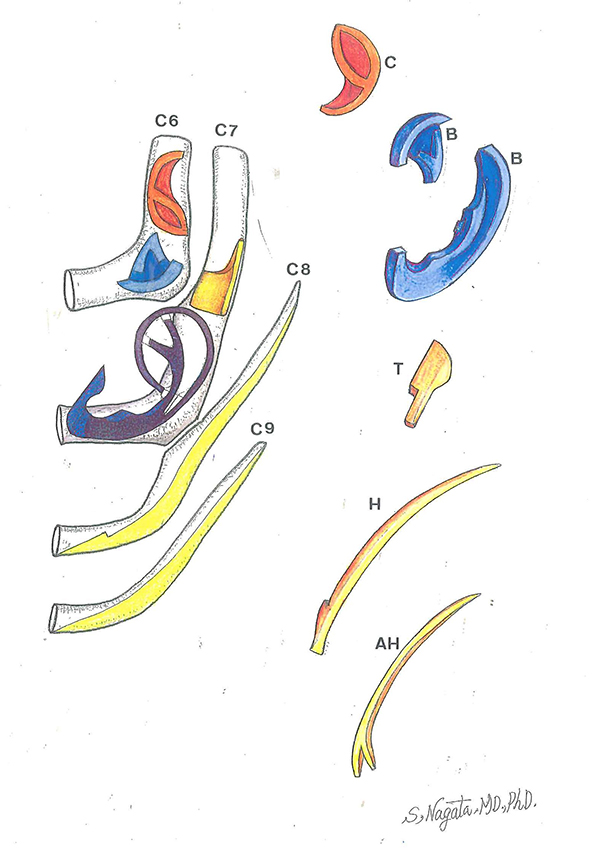
Fabrication of the 3-D frame. Diagrams C6, C7, C8 and C9: The costal cartilages harvested for the fabrication of the 3-D frame are the sixth [C6], seventh [C7], eighth [C8] and the ninth [C9] costal cartilages. Diagram C: This is the conchal vault unit of the 3-D frame; it is fabricated from the remaining costal cartilage after the fabrication of the base frame units and the tragus unit. There are occasions where the conchal vault unit is fabricated as two separate units, depending on the size of the remaining costal cartilage. Diagram B: The units for the fabrication of the base frame; these units are fabricated from the sixth and seventh costal cartilages. Diagram T: The tragal unit is fabricated from the largest remaining costal cartilage after the fabrication of the base frame units. Diagram H: This is the crus helices-helical rim unit and it is fabricated from the eighth costal cartilage. Diagram AH: the superior and inferior crus-antihelix unit which is fabricated from the ninth costal cartilage.
Fixation of the 3-D frame units.
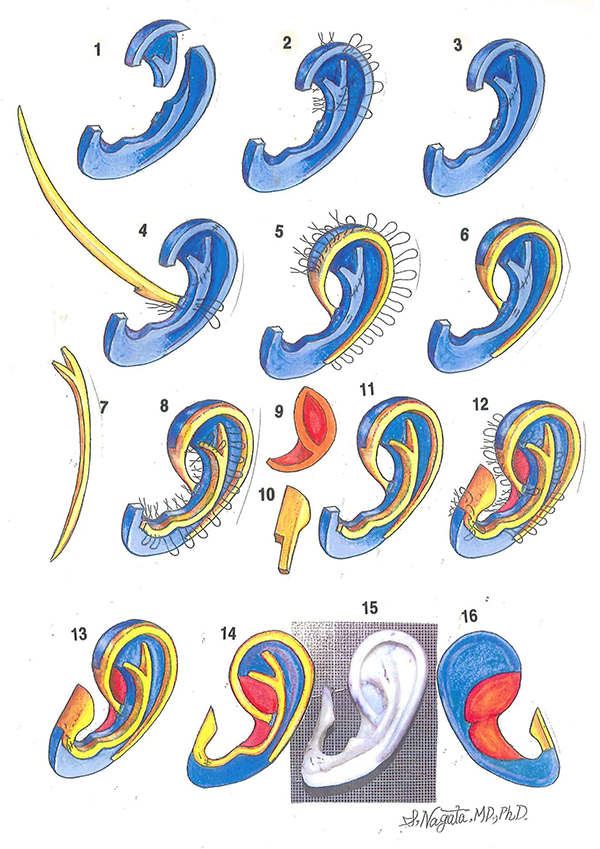
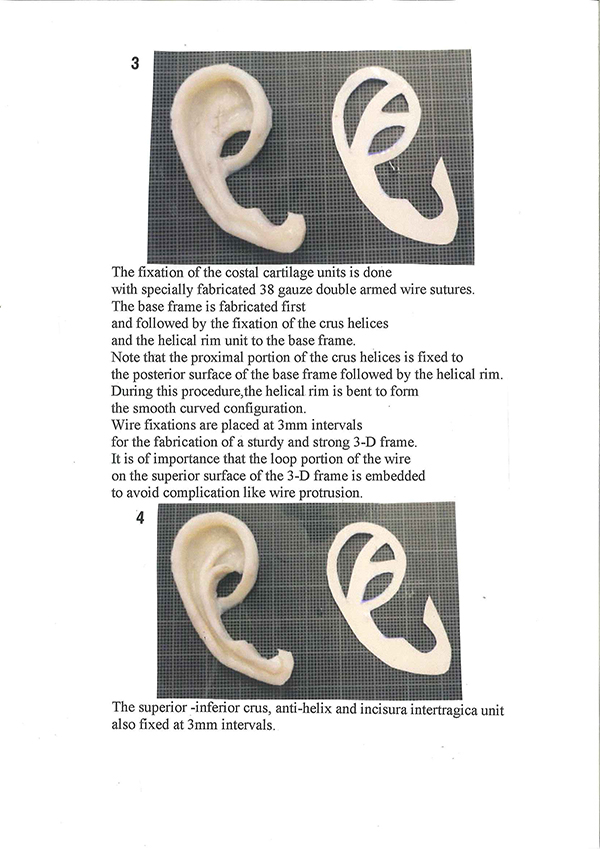
Diagram1 and 2: The base frame units are fixed with 38-gauge stainless steel double-armed wire sutures for a study and rigid fixation. Diagram 3: The fabricated base frame. Diagrams 4 and 5: The fixation of the crus helices-helical rim unit to the base frame. The head of the proximal region of the crus helicis is fixed to the posterior surface of the base frame and the notch is aligned to the base frame to reinforce the strength of the 3-D frame. Wire fixations are placed 3mm intervals. Note that the loop portion of the wire suture is embedded into the cartilage framework to avoid the postoperative complication of wire suture protrusion. Diagram 6: The appearance after the fixation of the crus helicis-helical rim unit to the base frame. Diagram 7: The superior and inferior-antihelix unit. Diagram 8: the fixation of the superior and inferior crus-antihelix unit, commencing from the superior crus, inferior crus to the antihelix. Diagram 9: The concal vault unit. Diagram10: The tragal unit. Diagram 11: The appearance after the fixation of the superior and inferior crus-antihelix unit. Diagram 12: The fixation of the tragal and conchal vault units to the 3-D frame. The tragal unit is fixed first, followed by the conchal vault unit. Diagram 13: illustrated angle view of the fabricated 3-D frame. Diagram 14: anterior view of the fabricated 3-D frame. Diagram 15: The anterior view of an actual 3-D frame. Diagram 16: The posterior view of the 3-D frame.
How to Fabricate 3D Costal Cartilage Framework
How to Fabricate Skin Flap for Lobule Type Microtia
First stage operation - lobule type microtia
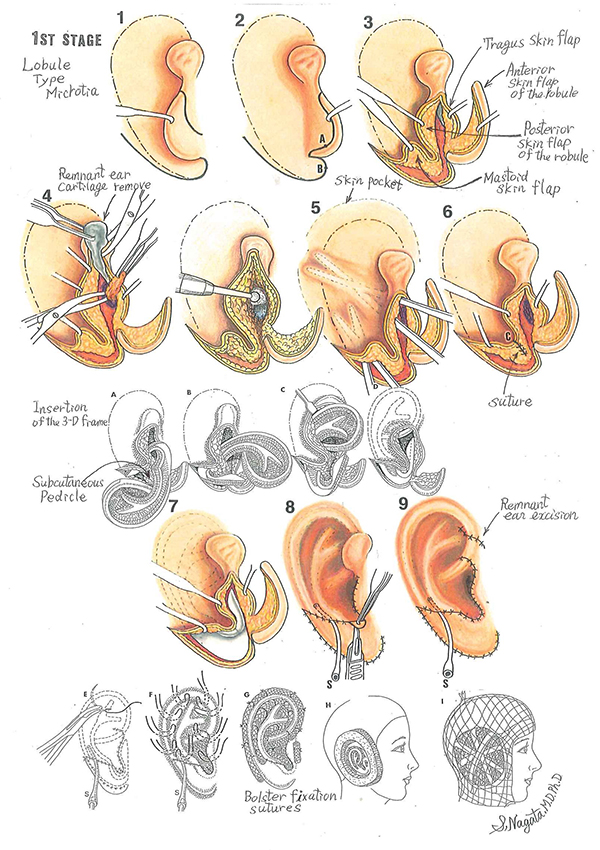
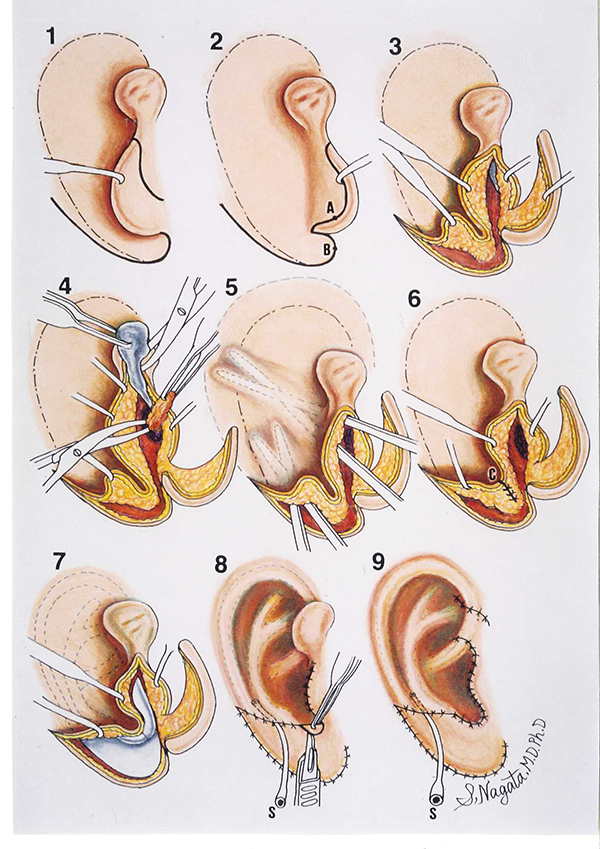
The surgical procedures for the first stage operation for lobule type microtia. Diagram 1: The outline of the auricle to be reconstructed and the incision outline for the anterior surface of the lobule. Diagram 2: The W-shaped incision outline on the posterior surface of the lobule and the mastoid surface. Note that the distal end of the W-shaped incision outline terminates 5 mm from the plotted outline of the auricle to be reconstructed. Diagram 3: The four skin flaps formed: the anterior and posterior skin flaps of the lobule, the anterior skin flap of the tragus and the mastoid skin flap. Diagram 4: The remnant auricular cartilage is completely removed and the soft tissue corresponding to the region of the auditory canal is excised to expose the periosteum. The periosteum is incised in a semi-circular fashion, sutured to the soft tissue of the parotid gland side in the form like a hinge flap to expose the temporal bone and then deepened with a burr. Diagram 5: The construction of the skin pocket, note that the undermining procedure extends 1cm beyond the outline area of the auricle. Diagram 6: The cone-shaped lining of the incisula intertragica is constructed by suturing points A and B. The inferior half of the posterior skin flap of the lobule and part of the mastoid skin flap are preserved to form the subcutaneous pedicle.
Diagram A, B, C and D: The 3-D frame is inserted under the skin cover from the tragal portion and centered with the subcutaneous pedicle. Diagram 7: The appearance after insertion of the 3-D frame under the skin cover. Diagram 8: Intraoperative suction is applied to visualize the contour and to adjust the skin cover over the 3-D frame after suturing of the skin flaps. The excessive skin at the incisula intertragica is excised in a semi-circular fashion to obtain the smooth U-shaped configuration of the intertragic notch. Diagram 9: The excessive skin [remnant ear] in the anterior helical region is excised and the suction is to be removed. Diagram E, F and G: Bolster sutures are placed in the indentations and around the helical rim of the reconstructed auricle. It is safe to place Bolster sutures, due to sufficient and ample skin surface area to cover the grafted 3-D frame. Diagram H: Restone foam sponge is cut out to surround the reconstructed auricle to provide protection. Diagram I: The illustrated appearance of the patient after the first stage auricular reconstruction operation.
The second stage operation - auricular projection
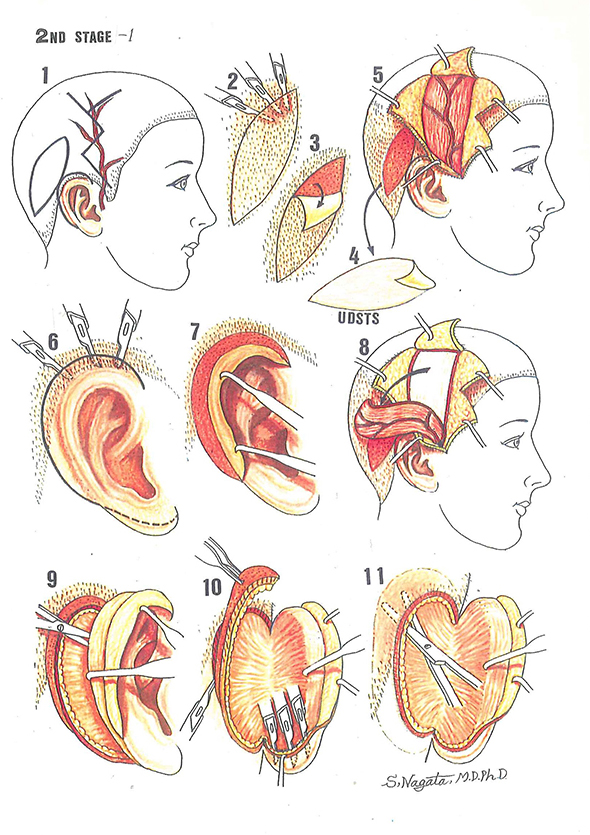
Schematic illustration of the second stage operation - auricular projection. Diagram1: The outline for the second stage operation, auricular projection. The spindle shape outline is for the harvesting of the ultra-delicate split-thickness scalp skin [UDSTS] and the outline along the helical rim is for the release of the reconstructed auricle. The zigzag outline is the incision outline for the elevation of the temporoparietal fascia flap [TPF] with the superficial temporal artery plotted. Diagram 2 and 3: The method of harvesting the UDSTS with a scalpel [number 15 blades]. Diagram 4 and 5: The harvested UDSTS with the area where it was harvested, and the preparation for the elevation for the TPF. Diagram 6: For the release of the reconstructed auricle, the area immediately adjacent to the helical rim which penetrates into the hair-bearing skin is elevated in the same manner as the UDSTS to the distance of 4 mm from the margin of the reconstructed auricle. Diagram 7: The follicular bud layer is left at the site of elevation of the UDSTS portion of the skin cover. Diagram 8: The elevated TPF. Diagram 9: The release of the reconstructed auricle from the site of the head. Diagram 10: The layer with the follicular buds adjacent to the helical rim is to be excised. Diagram 11: The skin of the temporal and mastoid surfaces is undermined.
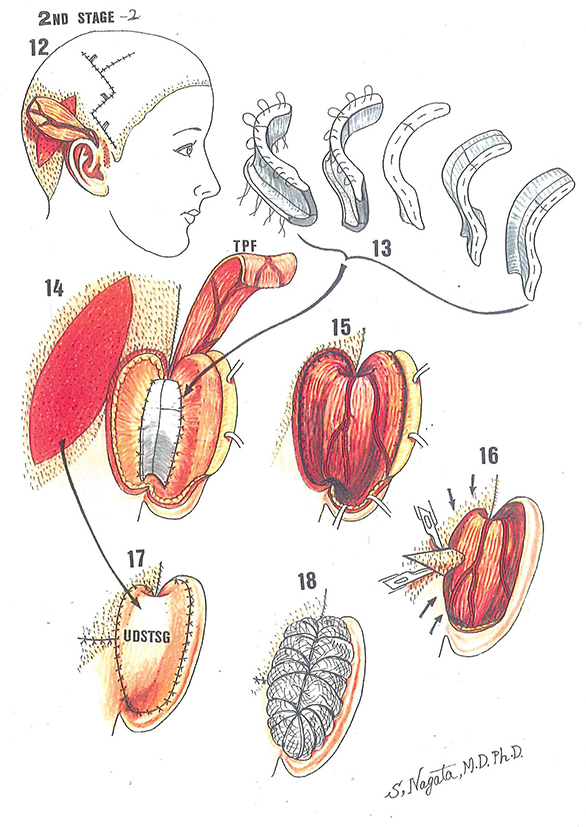
Diagram 12: The TPF is passed through the skin tunnel and the site of elevation is closed. Diagram 13: A simplified illustration of the costal cartilage construct with the modification in the inferior portion of the construct, reversed letter L configuration to increase stability. The cartilage block construct is multi-layered, and the units are fixed with 38-gauge wire sutures. Diagram 14: The cartilage block is fixed to the soft tissue of the posterior surface of 3-D frame and to the temporal and mastoid surfaces with 4-0 clear nylon. Diagram 15: The TPF covers the top of exposed helix [the UDSTS portion of the skin cover], the posterior surface of the reconstructed auricle, the cartilage block and the temporal and mastoid surfaces. Diagram 16: The skin of the temporal and mastoid surfaces is approximated and the excessive skin is excised in a triangular configuration in the hair-bearing skin to avoid dog ear formation. Diagram 17: The exposed surface is covered with the UDSTS. Diagram 18: The tie-over is performed to keep the UDSTS in contact to the TPF.
Fabrication of cartilage block for the second-stage surgery
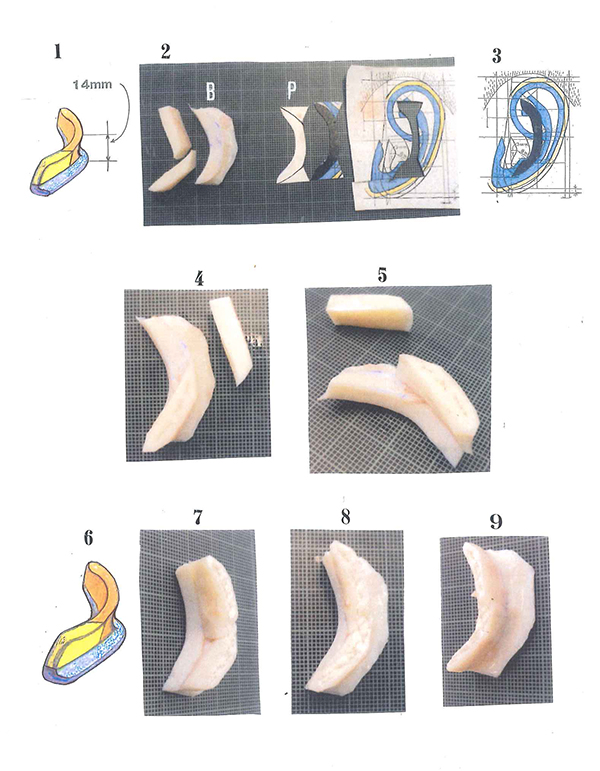
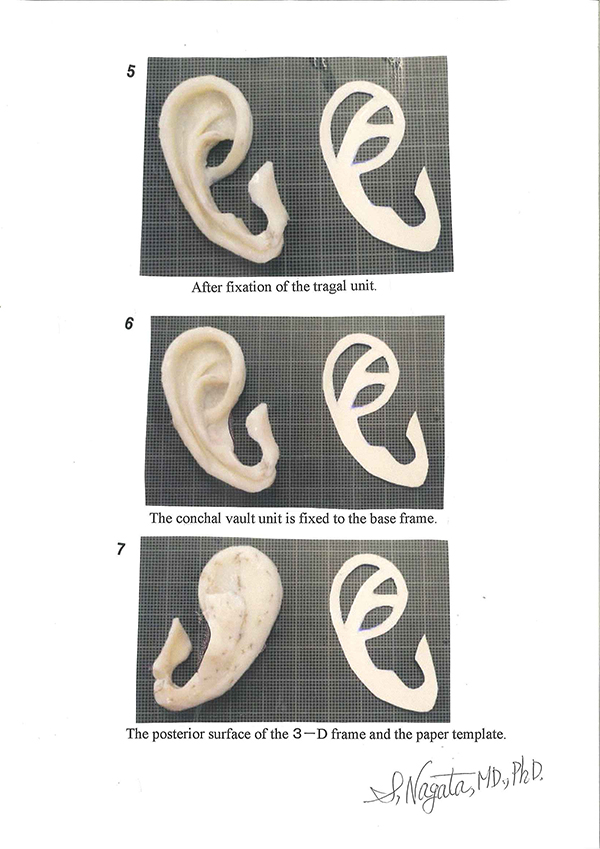
At the second-stage surgery, a crescent-shaped costal cartilage block is fabricated to support and project the reconstructed auricle. For bilateral microtia cases, the fourth and fifth costal cartilages from the same side as the first-stage surgery are harvested and used as the material for the fabrication of costal cartilage block. For unilateral microtia cases, the sixth and seventh costal cartilages from the opposite side may be used. Two (2) costal cartilages are placed on the base frame to fabricate a costal cartilage block with the thickness of 14 mm. See the Figure 1. The crescent-shaped part is cut out from the design shown in the Figure 3 to make a paper template. See the Figure 2-P. The base frame is fabricated with the same size as the paper template by placing it on the costal cartilage harvested. See the Figure 2-B. One of the two costal cartilages harvested is placed on the base frame and fixed with 38-gauge stainless wires. See the Figures 4 and 5. In the same way, another costal cartilage is placed on the base frame and fixed using the wires to complete the costal cartilage block. See the Figures 6, 7, 8 and 9. Figure 6 shows the illustration of costal cartilage block. Figures 7, 8 and 9 are an anterior-oblique view, a lateral view and a posterior-oblique view, respectively. The number of points fixed with the wire is 20.
History of Auricular Reconstruction
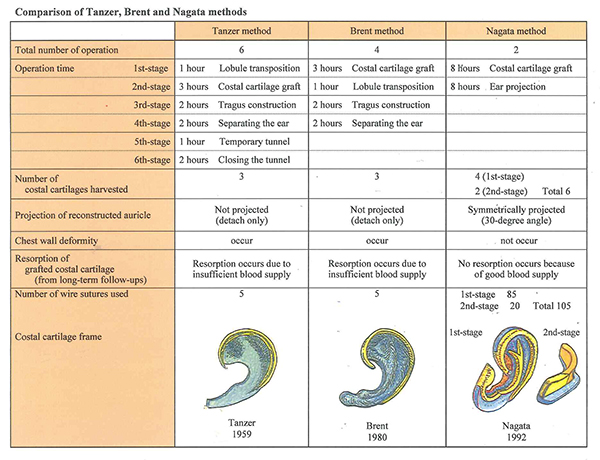
Ever since the introduction of autogenous auricular reconstruction by RC Tanzer of the United States, numerous developments, refinements, modifications for auricular reconstruction have been reported. The major auricular reconstruction methods known are the Tanzer method, Brent's method and the Nagata method,the Nagata method was developed and introduced in the mid 1980's.
One of the major differences among these 3 auricular reconstruction methods is in the number of surgeries required to reconstruct the auricle. The Tanzer method requires 6b surgeries, Brent’s method requires 4 surgeries and 2 surgeries for my method. The analyses of an ideal auricle reported by Hale Tolleth, MD, a prominent plastic surgeon in the United States, described in detail the anatomical features, proper anatomical location of the auricle, proportional and dimensional analyses of what an auricle must have to be an ear. When the reconstructed auricles by Tanzer and Brent were comparatively analyzed to what Tolleth had described in his analyses, there were numerous discrepancies noted to that of an ideal auricle. The Nagata method solved these discrepancies and as to the results, the proportional and dimensional analyses of the reconstructed auricle with my method ware within 1 to 2 percent deviation from what Tolleth had described as an ideal auricle.The projection of the reconstructed auricle which was not possible to attain with conventional auricular projection methods can now be attained with the method I developed.
Presently, the Nagata method is described in numerous American medical textbooks of Plastic Surgery and now accepted worldwide as one of the “Gold Standards” for total and subtotal auricular reconstruction.
Representative Auricular Reconstruction Cases-Primary Auricular Reconstruction
The representative cases for primary auricular reconstruction, patient who underwent auricular reconstruction for the first time are presented. The patients are generally children and the criteria established for the first stage operation are: minimum age of 10 years and chest circumference of at least 60 cm at the xiphoid process with both arms at the patient’s sides, X-ray confirmation of costal cartilage volume is required.
The classification of microtia is categorized into the following 4 types in reference to the severity of the microtic condition.
・Lobule Type
・Concha Type
・Small Concha Type
・Anotia
Representative Cases for Primary Auricular Reconstruction
Other than the above mentioned 4 types of microtia (non-complicated type), primary auricular reconstruction can be further complicated with conditions like low hairline. This condition is considered as a difficult auricular reconstruction case since if the auricle is reconstructed in the proper anatomical location the outcome result will be an auricle with hair growth (hairy auricle). With the conventional methods, the surgeon reconstructs a hairy auricle or will reconstruct the auricle in an abnormal anatomical location (usually in a lower anatomical location) to avoid the low hairline.
With the Nagata method, all these problems have been solved and it is possible to reconstruct the auricle in its proper anatomical location and without hair growth.















Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Representative Auricular Reconstruction Cases-Secondary Auricular Reconstruction







Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Cryptotia



Photos in this blog are shown for your reference for understanding ear reconstruction surgery. Please understand that surgery results vary depending on each case.
Possible complications following ear reconstruction surgery
Infection, Suture failure and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Stahl's ear




Photos in this blog are shown for your reference for understanding ear reconstruction surgery. Please understand that surgery results vary depending on each case.
Possible complications following ear reconstruction surgery
Infection, Suture failure and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Traumatic auricular defect


Photos in this blog are shown for your reference for understanding ear reconstruction surgery. Please understand that surgery results vary depending on each case.
Possible complications following ear reconstruction surgery
Infection, Suture failure and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Cup ear

Photos in this blog are shown for your reference for understanding ear reconstruction surgery. Please understand that surgery results vary depending on each case.
Possible complications following ear reconstruction surgery
Infection, Suture failure and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Lop Ear

Photos in this blog are shown for your reference for understanding ear reconstruction surgery. Please understand that surgery results vary depending on each case.
Possible complications following ear reconstruction surgery
Infection, Suture failure and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Traumatic auricular defect

Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.