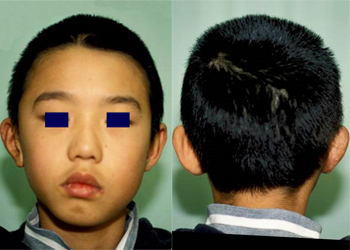
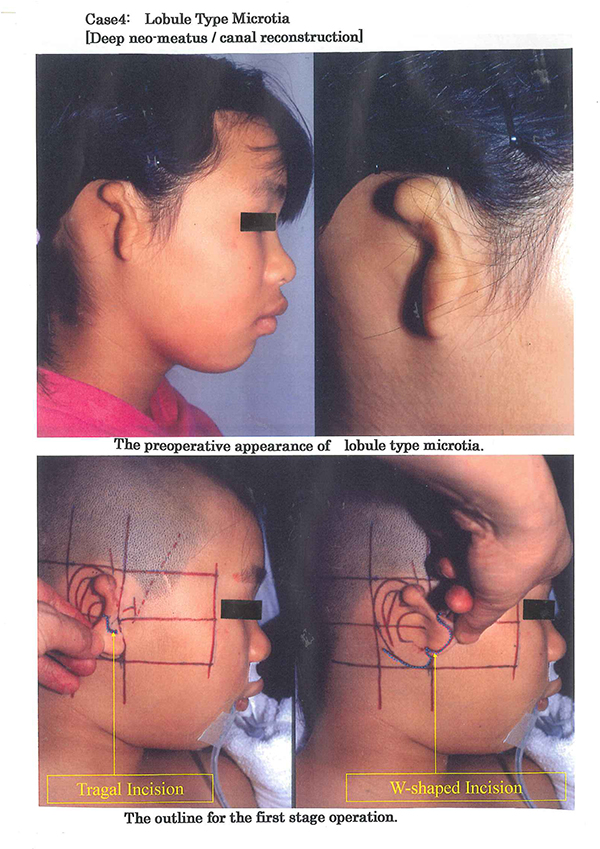
Preoperative appearance

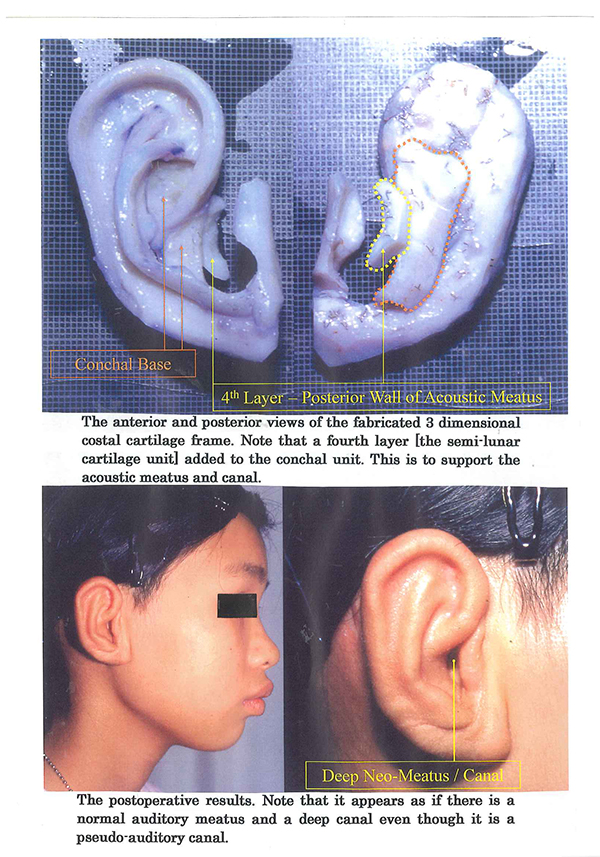
Post-operative appearance
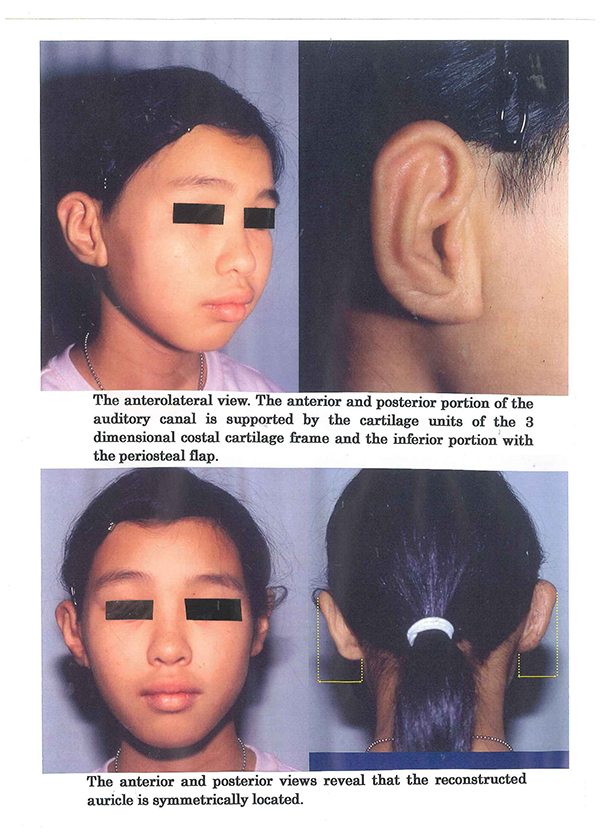
Post-operative appearance
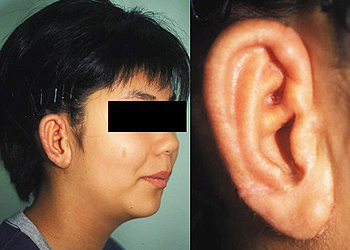
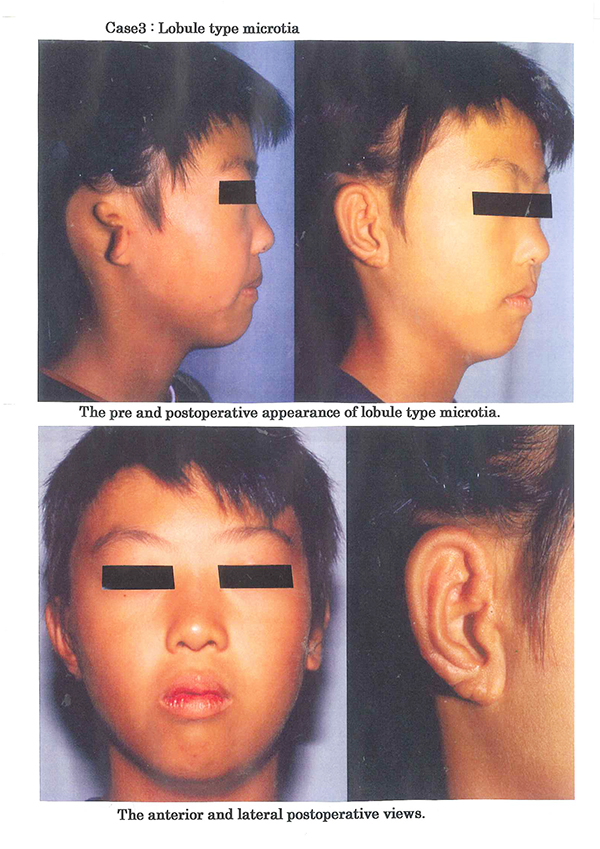
Typical lobule type microtia with the sausage-shaped vestige and there is no acoustic meatus and auditory canal. The patient is able to wear glasses after the second stage operation for auricular projection.
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
First stage operation-The fabrication of the 3 dimensional costal cartilage frame [3-D frame]
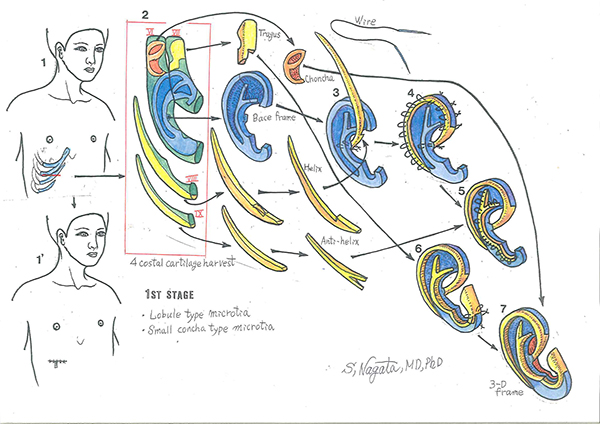
Diagram 1: The costal cartilages harvested for the fabrication of the 3-D frame are the sixth, seventh, eights, and the ninth costal cartilages. Diagram 2: Harvested 4 costal cartilages. The tragus unit, the base frame units, the crus helices-helical rim unit and the superior and inferior crus antihelix unit are fabricated from the costal cartilages. The units for the fabrication of the base frame; these units are fabricated from the sixth and seventh costal cartilages with 38 gauge stainless steel double-armed wire sutures. Diagram 3: The head of the proximal region of the crus helicis is fixed to the posterior surface of the base frame and the notch is aligned to the base flame to reinforce the strength of the 3-D frame. Diagram 4: Wire fixations are placed 3 mm intervals. Note that the loop portion of the wire sutures is embedded into the cartilage framework to avoid the postoperative complication of wire suture protrusion. Diagram 5: The fixation of the superior and inferior crus-antihelix unit, commencing from the superior crus, inferior crus, to the antihelix. Diagram 6: The appearance after the fixation of the tragus unit. Diagram 7: The appearance after the fixation of the conchal vault unit and completely fabricated 3-D frame.
First stage operation - lobule type microtia
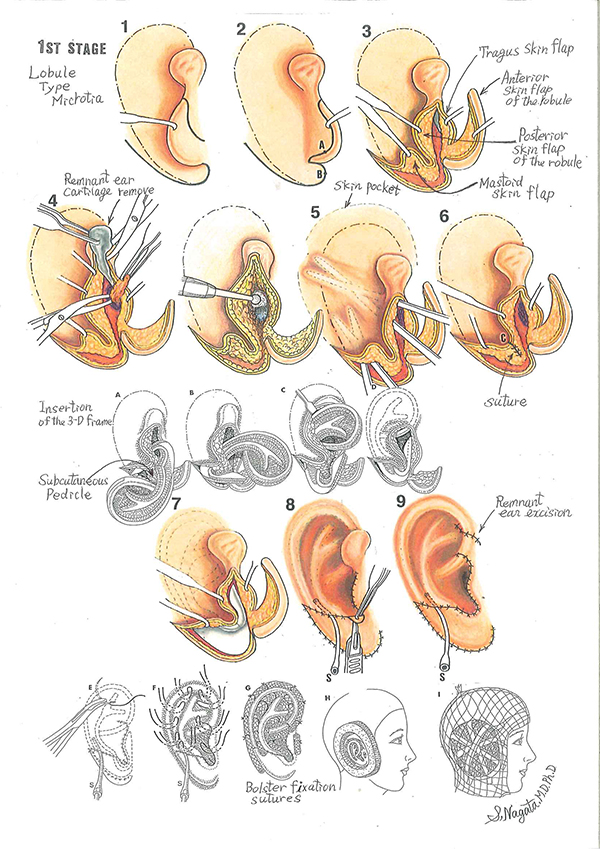
The surgical procedures for the first stage operation for lobule type microtia. Diagram 1: The outline of the auricle to be reconstructed and the incision outline for the anterior surface of the lobule. Diagram 2: The W-shaped incision outline on the posterior surface of the lobule and the mastoid surface. Note that the distal end of the W-shaped incision outline terminates 5 mm from the plotted outline of the auricle to be reconstructed. Diagram 3: The four skin flaps formed: the anterior and posterior skin flaps of the lobule, the anterior skin flap of the tragus and the mastoid skin flap. Diagram 4: The remnant auricular cartilage is completely removed and the soft tissue corresponding to the region of the auditory canal is excised to expose the periosteum. The periosteum is incised in a semi-circular fashion, sutured to the soft tissue of the parotid gland side in the form like a hinge flap to expose the temporal bone and then deepened with a burr. Diagram 5: The construction of the skin pocket, note that the undermining procedure extends 1cm beyond the outline area of the auricle. Diagram 6: The cone-shaped lining of the incisula intertragica is constructed by suturing points A and B. The inferior half of the posterior skin flap of the lobule and part of the mastoid skin flap are preserved to form the subcutaneous pedicle.
Diagram A, B, C and D: The 3-D frame is inserted under the skin cover from the tragal portion and centered with the subcutaneous pedicle. Diagram 7: The appearance after insertion of the 3-D frame under the skin cover. Diagram 8: Intraoperative suction is applied to visualize the contour and to adjust the skin cover over the 3-D frame after suturing of the skin flaps. The excessive skin at the incisula intertragica is excised in a semi-circular fashion to obtain the smooth U-shaped configuration of the intertragic notch. Diagram 9: The excessive skin [remnant ear] in the anterior helical region is excised and the suction is to be removed. Diagram E, F and G: Bolster sutures are placed in the indentations and around the helical rim of the reconstructed auricle. It is safe to place Bolster sutures, due to sufficient and ample skin surface area to cover the grafted 3-D frame. Diagram H: Restone foam sponge is cut out to surround the reconstructed auricle to provide protection. Diagram I: The illustrated appearance of the patient after the first stage auricular reconstruction operation.
The second stage operation - auricular projection
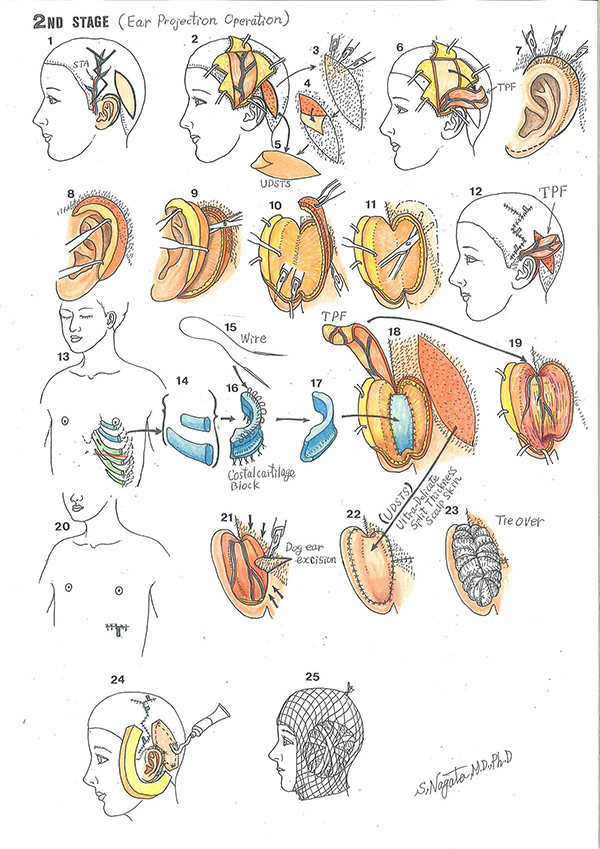
Schematic illustration of the second stage operation - auricular projection. Diagram 1: The outline for the second stage operation, auricular projection. The spindle shape outline is for the harvesting of the ultra-delicate split-thickness scalp skin [UDSTS] and the outline along the helical rim is for the release of the reconstructed auricle. The zigzag outline is the incision outline for the elevation of the temporoparietal fascia flap [TPF] with the superficial temporal artery plotted. Diagram 2 and 5: The harvested UDSTS with the area where it was harvested, and the preparation for the elevation for the TPF. Diagram 3 and 4: The method of harvesting the UDSTS with a scalpel [number 15 blades]. Diagram 6: The elevated TPF. Diagram 7: For the release of the reconstructed auricle, the area immediately adjacent to the helical rim which penetrates into the hair-bearing skin is elevated in the same manner as the UDSTS to the distance of 4 mm from the margin of the reconstructed auricle. Diagram 8: The follicular bud layer is left at the site of elevation of the UDSTS portion of the skin cover. Diagram 9: The release of the reconstructed auricle from the site of the head. Diagram 10: The layer with the follicular buds adjacent to the helical rim is to be excised. Diagram 11: The skin of the temporal and mastoid surfaces is undermined. Diagram 12: The TPF is passed through the skin tunnel and the site of elevation is closed. Diagram 13, 14: C4, C5 costal cartilage harvest. Diagram 15, 16, 17: A simplified illustration of the costal cartilage construct with the modification in the inferior portion of the construct, reversed letter L configuration to increase stability. The cartilage block construct is multi-layered, and the units are fixed with 38-gauge wire sutures. Diagram 18: The cartilage block is fixed to the soft tissue of the posterior surface of 3-D frame and to temporal and mastoid surfaces with 4-0 clear nylon. Diagram 19: The TPF covers the top of exposed helix [the UDSTS portion of the skin cover], the posterior surface of the reconstructed auricle, the cartilage block and the temporal and mastoid surfaces. Diagram 20: Skin suture line. Diagram 21: The skin of the temporal and mastoid surfaces is approximated and the excessive skin is excised in a triangular configuration in the hair-bearing skin to avoid dog ear configuration. Diagram 22: The exposed surface is covered with the UDSTS. Diagram 23: The tie-over is performed to keep the UDSTS in contact to the TPF. Diagram 24: Restone foam sponge is cut out to the reconstructed auricle to provide protection. Diagram 25: The illustrated appearance of the patient after the second stage operation.


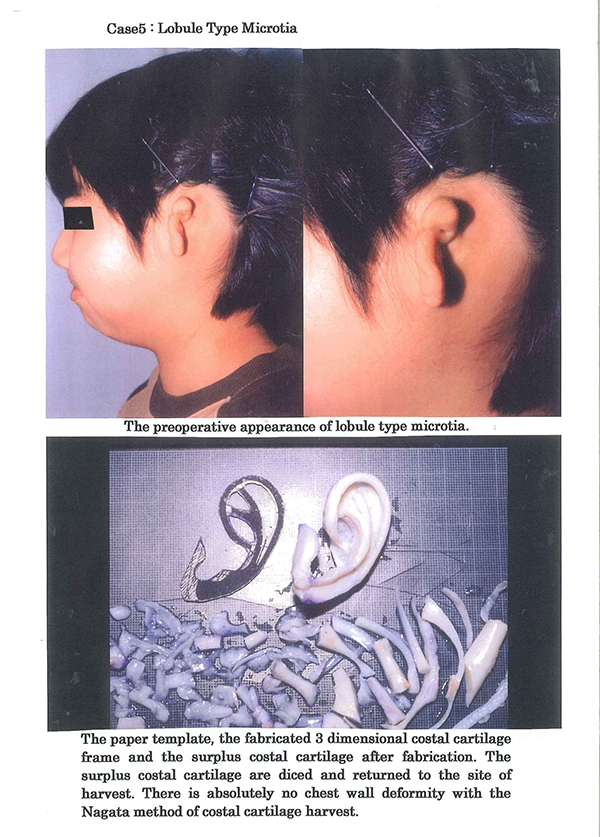
Preoperative appearance
Post-operative appearance
Before the operation:
The same microtia classification as Case 1 but of the right side with the sausage-shaped vestige and there is no acoustic meatus and auditory canal.
After the first-stage operation:
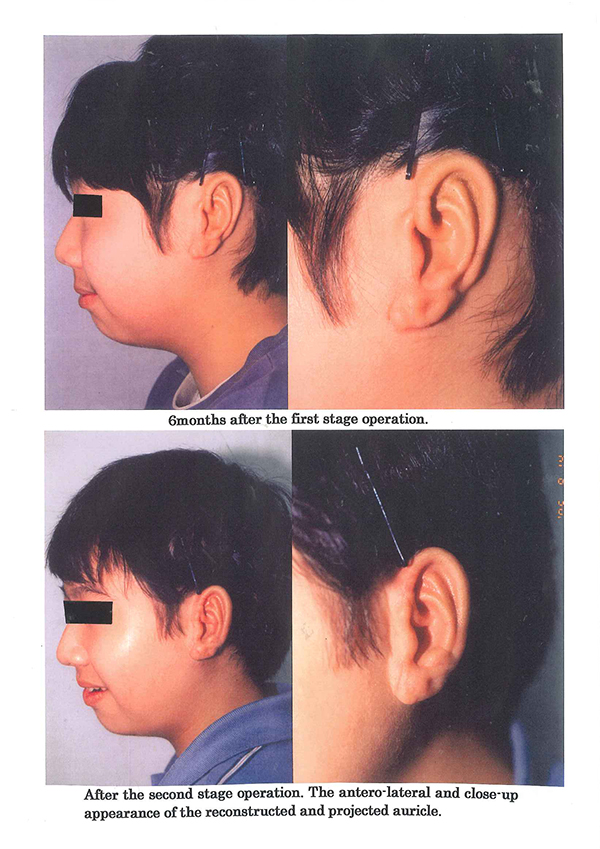
Appearance at 6 months after the first stage operation and immediately prior to the second stage operation for auricular projection. Note that the morphological features of the auricle have been reconstructed.
After the second-stage operation:
Appearance after the second stage operation, the reconstructed auricle is projected.
After the second-stage operation:
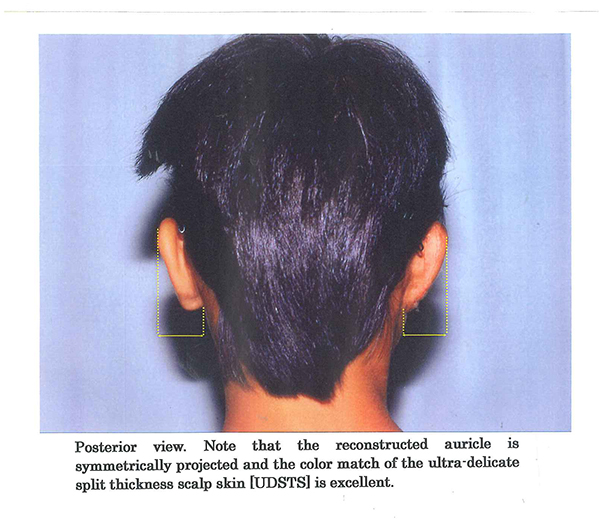
Follow-up appearance of the same patient after auricular projection. The projected auricle is well maintained and there appears as if there is an acoustic meatus beneath the constructed tragus.
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.

Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.
Photos in this blog are shown for your reference for understanding the treatment of microtia. Please understand that surgery results vary depending on each case.
Possible complications following microtia reconstruction surgery
Transient facial palsy, Failure of skin graft due to vascular compromise, Infection resulting in exposure of the 3-D frame, Pneumothorax, Postoperative pneumonia, Suture failure, Alopecia, Decubitus and Others
In the event such complications arise, appropriate action is taken based on the case. Additional or secondary surgery may be required in some situations.

Click here for “1st-stage operation for lobule type microtia” conducted on Feb. 24, 2015 for reference.